Will Over-Pronation Of The Foot Need To Have Surgical Treatment
Overview
Pronation or eversion is the inward roll of the foot while walking or running. Another way to look at pronation instead in terms of the degree of inward roll is in terms of where the foot pushes off at the end of each step, or at the end of the gait cycle. There are three main types of pronation in human gait: neutral pronation, overpronation, and underpronation or supination. While both overpronation and supination occur while walking and standing, they are usually more pronounced and the effects amplified while running. Those who overpronate tend to push off almost completely from the big toe and second toe. As a result, the shock from the foot?s impact doesn?t spread evenly throughout the foot and the ankle has trouble stabilizing the rest of the body. Additionally, an unnatural angle forms between the foot and ankle and the foot splays out abnormally. It is common even for people who pronate normally to have some angle between the foot and the ankle, but not to the extent seen in those who overpronate. In normal pronation the weight distributes evenly throughout the foot.
Causes
Although there are many factors that can contribute to the development of these conditions, improper biomechanics of the body plays a large and detrimental role in the process. Of the many biomechanical elements involved, foot and ankle function perhaps contribute the most to these aches and pains.
Symptoms
Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.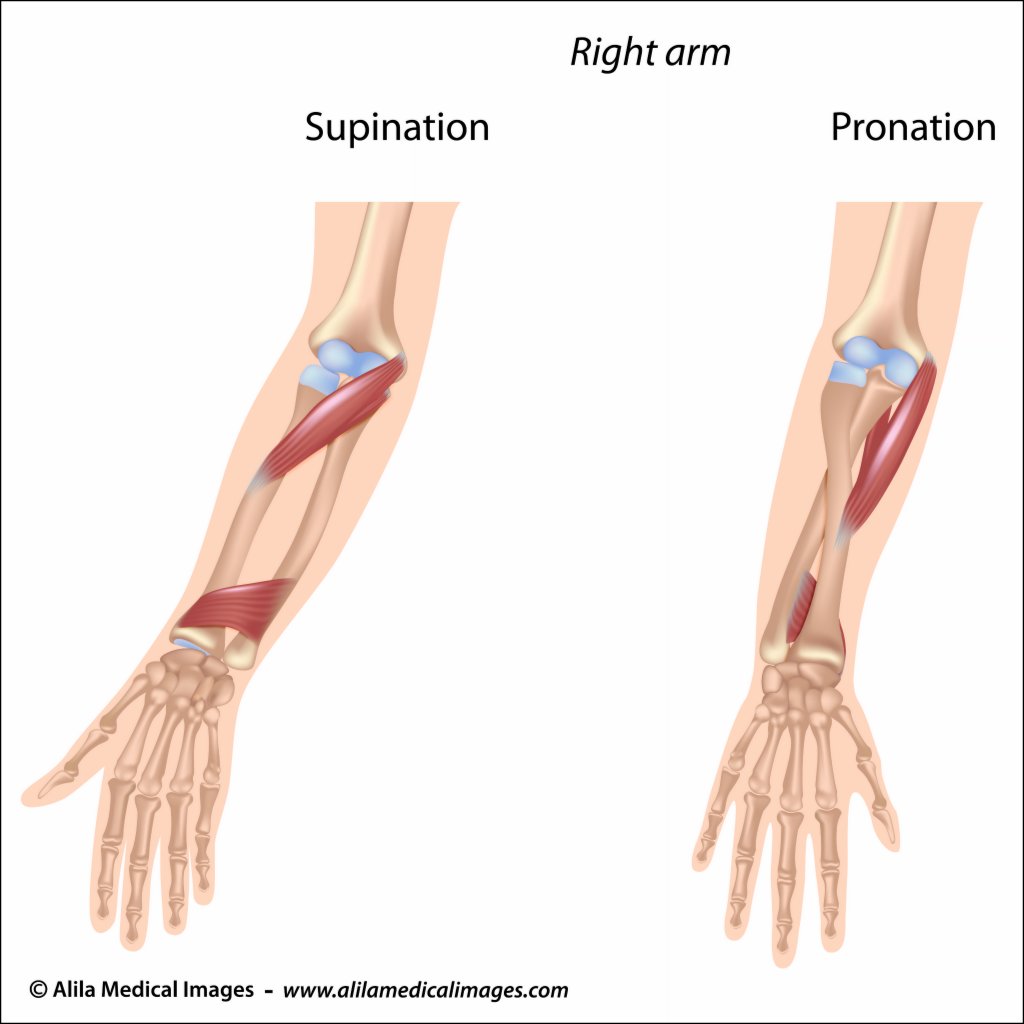
Non Surgical Treatment
Studies have shown that the most effective way to dexrease a high Q angle and lower the biomechanical stresses on the knee joint is to prevent excessive pronation with custom-maflexible orthotics. One study found that using soft corrective orthotics was more effective in reduknee pain than a traditional exercise program. A more recent study showed that Q angle asymmetries, secondary to excessive pronation affecting knee alignment, can be effectivecontrolled or corrected utilizing custom-made, flexible orthotics. Another project involving meof a running club determined that 75% of those using orthotics eliminated or greatly reduced pain in the feet, ankles, shins, knees and hips
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.
Pronation or eversion is the inward roll of the foot while walking or running. Another way to look at pronation instead in terms of the degree of inward roll is in terms of where the foot pushes off at the end of each step, or at the end of the gait cycle. There are three main types of pronation in human gait: neutral pronation, overpronation, and underpronation or supination. While both overpronation and supination occur while walking and standing, they are usually more pronounced and the effects amplified while running. Those who overpronate tend to push off almost completely from the big toe and second toe. As a result, the shock from the foot?s impact doesn?t spread evenly throughout the foot and the ankle has trouble stabilizing the rest of the body. Additionally, an unnatural angle forms between the foot and ankle and the foot splays out abnormally. It is common even for people who pronate normally to have some angle between the foot and the ankle, but not to the extent seen in those who overpronate. In normal pronation the weight distributes evenly throughout the foot.
Causes
Although there are many factors that can contribute to the development of these conditions, improper biomechanics of the body plays a large and detrimental role in the process. Of the many biomechanical elements involved, foot and ankle function perhaps contribute the most to these aches and pains.
Symptoms
Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
Studies have shown that the most effective way to dexrease a high Q angle and lower the biomechanical stresses on the knee joint is to prevent excessive pronation with custom-maflexible orthotics. One study found that using soft corrective orthotics was more effective in reduknee pain than a traditional exercise program. A more recent study showed that Q angle asymmetries, secondary to excessive pronation affecting knee alignment, can be effectivecontrolled or corrected utilizing custom-made, flexible orthotics. Another project involving meof a running club determined that 75% of those using orthotics eliminated or greatly reduced pain in the feet, ankles, shins, knees and hips
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.
What Exactly Is Severs Disease?
Overview
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
Apart from the age of the young person, other factors that may contribute to developing the disease may include; overuse or too much physical activity. Your child?s heel pain may be caused by repeated stress on the heels (running and jumping activities), pressure on the back of the heel from too much standing or wearing poor-fitting shoes. This includes shoes that do not support or provide enough padding for your child?s feet.
Symptoms
Activity-related pain that occurs on the back of the heel, where the Achilles tendon attaches on to the heel bone. Tenderness, pain & swelling on the heel bone. Difficulty walking or walking with a limp or on tiptoes.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
The doctor might recommend that a child with Sever's disease. perform foot and leg exercises to stretch and strengthen the leg muscles and tendons, elevate and apply ice (wrapped in a towel, not applied directly to the skin) to the injured heel for 20 minutes two or three times per day, even on days when the pain is not that bad, to help reduce swelling, use an elastic wrap or compression stocking that is designed to help decrease pain and swelling, take an over-the-counter medicine to reduce pain and swelling, such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin).
Recovery
Recovery time will vary from patient to patient. Age, health, previous injuries, and severity of symptoms will affect recovery time. Your compliance with the stretching program and the other recommendations made by your doctor will also determine your healing time. Heel pain often completely resolves after a child?s heel bone has stopped its period of growth.
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
Apart from the age of the young person, other factors that may contribute to developing the disease may include; overuse or too much physical activity. Your child?s heel pain may be caused by repeated stress on the heels (running and jumping activities), pressure on the back of the heel from too much standing or wearing poor-fitting shoes. This includes shoes that do not support or provide enough padding for your child?s feet.
Symptoms
Activity-related pain that occurs on the back of the heel, where the Achilles tendon attaches on to the heel bone. Tenderness, pain & swelling on the heel bone. Difficulty walking or walking with a limp or on tiptoes.
Diagnosis
Physical examination varies depending on the severity and length of involvement. Bilateral involvement is present in approximately 60% of cases. Most patients experience pain with deep palpation at the Achilles insertion and pain when performing active toe raises. Forced dorsiflexion of the ankle also proves uncomfortable and is relieved with passive equinus positioning. Swelling may be present but usually is mild. In long-standing cases, the child may have calcaneal enlargement.
Non Surgical Treatment
The doctor might recommend that a child with Sever's disease. perform foot and leg exercises to stretch and strengthen the leg muscles and tendons, elevate and apply ice (wrapped in a towel, not applied directly to the skin) to the injured heel for 20 minutes two or three times per day, even on days when the pain is not that bad, to help reduce swelling, use an elastic wrap or compression stocking that is designed to help decrease pain and swelling, take an over-the-counter medicine to reduce pain and swelling, such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin).
Recovery
Recovery time will vary from patient to patient. Age, health, previous injuries, and severity of symptoms will affect recovery time. Your compliance with the stretching program and the other recommendations made by your doctor will also determine your healing time. Heel pain often completely resolves after a child?s heel bone has stopped its period of growth.
What Will Be The Indications Of A Ruptured Achilles Tendon?
Overview
 A rupture of the Achilles tendon is one of the more common types of tendon ruptures. As the largest tendon in the human body, the Achilles tendon is very important to one?s balance and stability. Patients who suffer an Achilles tendon rupture experience severe pain and often require Achilles tendon surgery to repair the damage. There are also less invasive methods of Achilles tendon treatment including, icing, anti-inflammatory medications, rehabilitation, taping or bracing, sports massages and more. Achilles tendon recovery is dependent on the health of the patient, and the severity of the injury.
A rupture of the Achilles tendon is one of the more common types of tendon ruptures. As the largest tendon in the human body, the Achilles tendon is very important to one?s balance and stability. Patients who suffer an Achilles tendon rupture experience severe pain and often require Achilles tendon surgery to repair the damage. There are also less invasive methods of Achilles tendon treatment including, icing, anti-inflammatory medications, rehabilitation, taping or bracing, sports massages and more. Achilles tendon recovery is dependent on the health of the patient, and the severity of the injury.
Causes
Achilles tendon rupture occurs in people that engage in strenuous activity, who are usually sedentary and have weakened tendons, or in people who have had previous chronic injury to their Achilles tendons. Previous injury to the tendon can be caused by overuse, improper stretching habits, worn-out or improperly fitting shoes, or poor biomechanics (flat-feet). The risk of tendon rupture is also increased with the use of quinolone antibiotics (e.g. ciprofloxacin, Levaquin).
Symptoms
Patients with an Achilles tendon rupture will often complain of a sudden snap in the back of the leg. The pain is often intense. With a complete rupture, the individual will only be ambulate with a limp. Most people will not be able to climb stairs, run, or stand on their toes. Swelling around the calf may occur. Patients may often have had a sudden increase in exercise or intensity of activity. Some patients may have had recent corticosteroid injections or use of fluoroquinolone antibiotics. Some athletes may have had a prior injury to the tendon.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Non Surgical Treatment
Treatment of a ruptured Achilles tendon is usually conservative (non-operative) in a Controlled Motion Ankle (CAM) Boot or it may require surgery. The current consensus based on research is to treat them conservatively since the functional outcome and chance of re-rupture is similar (7% to 15%) using both approaches but surgical intervention has a higher risk of infection. Achilles tendon surgery is usually considered if your Achilles has re-ruptured or there is delay of two weeks between the rupture and the diagnosis and commencement of conservative bracing and treatment. 
Surgical Treatment
Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks.
Prevention
You can help to reduce your risk of an injury to your Achilles tendon by doing the following. When you start a new exercise regime, gradually increase the intensity and the length of time you spend being active. Warm up your muscles before you exercise and cool them down after you have finished. The benefit of stretching before or after exercise is unproven. However, it may help to stretch your calf muscles, which will help to lengthen your Achilles tendon, before you exercise. Wear appropriate and well-fitting shoes when you exercise.
Apparent Leg Length Discrepancy Causes
Overview
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
To begin a path torwards a balanced foundation and reduce pain from leg length discrepancy, ask your doctor about these Functional Orthotics and procedures. Functional Orthotics have been shown to specifically reduce pain from leg length inequality, support all three arches of the foot to create a balanced foundation, maximize shock absorption, add extra propulsion, and supply more stability, enable posture correction and long-term preventive protection. Will improve prolonged effectiveness of chiropractic adjustments. Shoe or heel Lifts, Correct the deficiencies that causes imbalances in the body.

Surgical Treatment
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
To begin a path torwards a balanced foundation and reduce pain from leg length discrepancy, ask your doctor about these Functional Orthotics and procedures. Functional Orthotics have been shown to specifically reduce pain from leg length inequality, support all three arches of the foot to create a balanced foundation, maximize shock absorption, add extra propulsion, and supply more stability, enable posture correction and long-term preventive protection. Will improve prolonged effectiveness of chiropractic adjustments. Shoe or heel Lifts, Correct the deficiencies that causes imbalances in the body.
Surgical Treatment
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
Cure For Flat Feet In Adults
Overview
Flatfoot deformity is a general term used to describe a person whose arches are slowly dropping to the ground, aka ?fallen arches.? Adult-acquired flatfoot deformity can be caused by several factors, but the most common is abnormal functioning of the posterior tibial tendon in the foot and ankle. The posterior tibial tendon is the primary tendon that supports the arch. If this tendon begins to elongate from a sustained, gradual stretch over a long period of time, then the arch will progressively decrease until full collapse of the arch is noted on standing. What makes this tendon elongated? Biomechanical instability of the foot such as over-pronation or an accessory bone at the insertion site of the tendon are the primary causes for posterior tibial tendon dysfunction. 
Causes
As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
Most people will notice mild to extreme pain in their feet. Below outlines some signs and symptoms of AAFD. Trouble walking or standing for any duration. Pain and swelling on the inside of the ankle. Bump on the bottom of the foot. Ulcer or wound developing on the outer aspects of foot.
Diagnosis
Although you can do the "wet test" at home, a thorough examination by a doctor will be needed to identify why the flatfoot developed. Possible causes include a congenital abnormality, a bone fracture or dislocation, a torn or stretched tendon, arthritis or neurologic weakness. For example, an inability to rise up on your toes while standing on the affected foot may indicate damage to the posterior tibial tendon (PTT), which supports the heel and forms the arch. If "too many toes" show on the outside of your foot when the doctor views you from the rear, your shinbone (tibia) may be sliding off the anklebone (talus), another indicator of damage to the PTT. Be sure to wear your regular shoes to the examination. An irregular wear pattern on the bottom of the shoe is another indicator of acquired adult flatfoot. Your physician may request X-rays to see how the bones of your feet are aligned. Muscle and tendon strength are tested by asking you to move the foot while the doctor holds it.
Non surgical Treatment
Options range from shoe inserts, orthotics, bracing and physical therapy for elderly and/or inactive patients to reconstructive surgical procedures in those wishing to remain more active. These treatments restore proper function and alignment of the foot by replacing the damaged muscle tendon unit with an undamaged, available and expendable one, lengthening the contracted Achilles tendon and realigning the Os Calcis, or heel bone, while preserving the joints of the hindfoot. If this condition is not recognized before it reaches advanced stages, a fusion of the hindfoot or even the ankle is necessary. Typically this is necessary in elderly individuals with advanced cases that cannot be improved with bracing. 
Surgical Treatment
If conservative treatment fails to provide relief of pain and disability then surgery is considered. Numerous factors determine whether a patient is a surgical candidate. They include age, obesity, diabetes, vascular status, and the ability to be compliant with post-operative care. Surgery usually requires a prolonged period of nonweightbearing immobilization. Total recovery ranges from 3 months to one year. Clinical, x-ray, and MRI examination are all used to select the appropriate surgical procedure.